


Weekly TMS Pulse
This Week
in TMS.
Stories + Heart · Science + Access · Every week.
The Treatment Gap
~33% · 5+ years
about one in three U.S. adults with major depression don’t respond to standard antidepressants — and most wait years before a provider even mentions TMS as an option.
The treatment exists. The evidence is settled. What’s missing is the conversation — and that’s the gap FACTMS exists to close.
Source: NIMH STAR*D outcomes (Rush et al., Am J Psychiatry, 2006); APA practice trend data, 2024
⚡ Brain Spark · Myth vs. Fact
Myth: “TMS is just another name for shock therapy (ECT).” Fact: TMS and ECT are completely different. TMS uses focused magnetic pulses to stimulate a small region of the brain; patients are awake, alert, and drive themselves home. There is no anesthesia, no induced seizure, and no memory loss. TMS has been FDA-cleared for major depression since 2008 and is now covered by most major insurers.
Source: U.S. FDA device clearance summaries; Yale Medicine TMS overview, 2025
The Heart
Patient Stories & Voices This Week
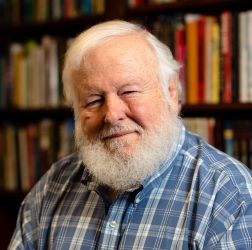
A NAMI Leader Shares Her Accelerated TMS Journey — “It Gave Me Back My Capacity for Joy”
Barb Solish, NAMI’s National Director of Innovation, has lived with anxiety and depression since she was a child and was diagnosed with bipolar II in her twenties. After a profound loss sent her into one of the darkest periods of her life — with serious suicidal thoughts — a psychiatrist recommended accelerated TMS (aTMS), using a 5-day protocol delivering multiple short sessions each day. Within days, Solish says her brain “just worked better,” and she published her story on NAMI’s blog so others could hear about a treatment she wishes she’d known about sooner. Note: TMS is FDA-cleared for major depressive disorder. Its use in bipolar II depression is off-label; patients should discuss options with their provider.
Why it matters
When a national mental-health leader — someone whose work is knowing every option in the landscape — says she wishes she’d heard about TMS sooner, it tells you how invisible this treatment still is. If TMS can surprise her, imagine how many others are suffering without ever hearing it exists.
Barb
NAMI National Director of Innovation · Bipolar II · Accelerated TMS recipient
NAMI Blog, April 2026
Barb found TMS. Most people in her position never do — and the barriers between patients and treatment are finally starting to fall.
Awareness & Access
Making TMS Known & Accessible
More Providers, More Access: UnitedHealthcare Lets Nurse Practitioners Deliver TMS
Optum / UnitedHealthcare / United Behavioral Health updated its TMS clinical policy to let psychiatric mental health nurse practitioners (PMHNPs) — not only psychiatrists — order, supervise, and administer TMS therapy. The change spans 26 states and Washington, D.C., reaching roughly 34.8 million covered lives, in states that grant nurse practitioners full practice authority. Until now, that authority sat with psychiatrists alone — a real bottleneck in regions where psychiatrists are scarce.
Why it matters
Coverage only helps if someone nearby can actually deliver the treatment. In rural and underserved areas, psychiatrists can be hours away or booked months out — while nurse practitioners are often the backbone of mental-health care. Letting PMHNPs run TMS widens the front door for millions of people who technically had coverage but no practical way to use it. It’s a quiet, structural change that turns “covered” into actually available.
Wider access gets more people through the door. New data this week asks the question patients care about most: once TMS works, does it last?
The Head
What the Research Says This Week
Does It Last? Accelerated TMS Holds at One Year — 80%+ Still in Remission
At the Clinical TMS Society annual meeting (June 4–6, 2026), BrainsWay presented the first 12-month durability data from the SWIFT trial — the first multisite randomized controlled trial of its accelerated Deep TMS protocol. Among patients followed a full year, over 80% remained in remission, and severe functional impairment fell from 85% at baseline to 0%. Fewer than 25% needed a medication change or another course of TMS within the year. SWIFT compresses the acute course, cutting in-clinic visits by about 70% versus the standard daily protocol — and the durable results held for standard once-daily Deep TMS too. Presented by Colleen Hanlon, PhD, VP of Medical Affairs.
Why it matters
The first question most patients ask about any depression treatment is “will it come back?” One-year data showing most people staying well — after a course that’s faster and needs far fewer visits — is exactly the evidence that makes accelerated TMS a realistic option for people who can’t take six weeks of daily appointments. The data are preliminary and industry-presented (not yet peer-reviewed), but the durability signal is a strong one.
From FACTMS
Share Your TMS Story — And Help Someone Else Find It Sooner
Patient stories are how most people first hear of TMS. If TMS changed your life — or a loved one’s — consider sharing it with FACTMS. Submitted stories may be featured on factms.org and in this newsletter (with your permission and on your terms), so the next person who is exhausted, out of options, and quietly looking for hope can find a story that sounds like theirs.
Share Your Story →Editorial Note
This newsletter is drafted with the assistance of AI and reviewed by the FACTMS editorial team. All sources are verified and linked. We take accuracy seriously — if something doesn’t look right, please let us know at info@factms.org.